
We’ve all been there. We’ve all used a piece of equipment or clinical software and thought, if only the developers and engineers understood how a hospital worked. Now there’s a growing community of clinicians who can code. The interesting thing is that they are now saying, if only other clinicians understood tech. I don’t mean that they want other clinicians to know how to code, they just want them to vaguely understand the basics of computer systems. I myself was naive when I got to grips with scripting in high-level languages. I thought that I could explain the advantages of certain scripts and data storage choices and the adoption would be quick, cheap and painless. The idea behind clinicians coding is that they could generate programs in high-level languages quickly that solve particular problems, they could then quickly refine them when problems came to their attention. The main inhibition I have seen is other clinicians not knowing anything about computers or computer systems whilst not admitting it. Of course, I don’t mean all clinicians are like this. I have come across my fair share of clinicians who openly admit that they don’t know anything about computers and will happily allow someone else to take the reigns, but the problem is more common than it should be. Below are two scary examples that keep arising for members in my coding groups.

data storage
This is the most widespread problem I come across. I understand why Excel is widely used, it’s easy to read and input data. Sadly that’s it’s only advantages. It’s slow, you cannot make multiple data requests at the same time and it will start to crash if you put too much data on it. It supports a limited range of data types. And calculations are not very precise, in terms of big data you are going to get errors. You will get some slight upgrades with these problems with Access, but again it’s not great. SQL based databases can handle multiple requests at the same time. They can serve the data over multiple computers, and support multiple data type inputs. This means that you can assign and store stuff like images to data objects in the database. You can also export the data into an Excel or CSV file if you need to send it to someone who is tech illiterate Considering that SQLite and SQL software is free to download and use the only reason you would pick the Microsoft packages over them is because you do not have the skill to code these database structures. That’s a valid reason, however, if someone is offering to code the structure for free then it’s just arrogance, combined with a lack of tech knowledge. One clinician from one of my coding groups offered to code an SQL database structure for logging surgeries. Even after meeting with them the consultants still insisted that the logging of surgeries should be done in Excel. This may seem rash but we have to conclude that their arrogance and lack of understanding is holding back their department as they turn down a free upgrade.
Strong opinions with little understanding
Because the average clinician is not educated in tech and has not sat any assessments in tech the bar for being a computer whizz is set very low. I’ve seen clinicians been branded whizzes because they can create macros in Excel. This is nothing more than cute compared to the skills that are being developed in these clinical coding clubs. However, these self-proclaimed computer whizzes have enjoyed the status and will not let reality threaten it. I have come across senior clinicians who state that they are tech savvy, and they want to innovate with tech. When I speak to them their titles are a result of being able to use Excel and having an interest in using social media to spread medical education. I’m not joking, I’ve met consultants who describe themselves as tech-orientated innovators (not branding leaders) who give presentations on how to use twitter. Whenever you speak to them they are incredibly dismissive, will try and break away from the conversation as quickly as possible. Basically, anything they don’t understand (which is a lot) is not even worth discussing. One example of this is machine learning. A neural network is where multiple different variables and be weighed against the probability calculation.
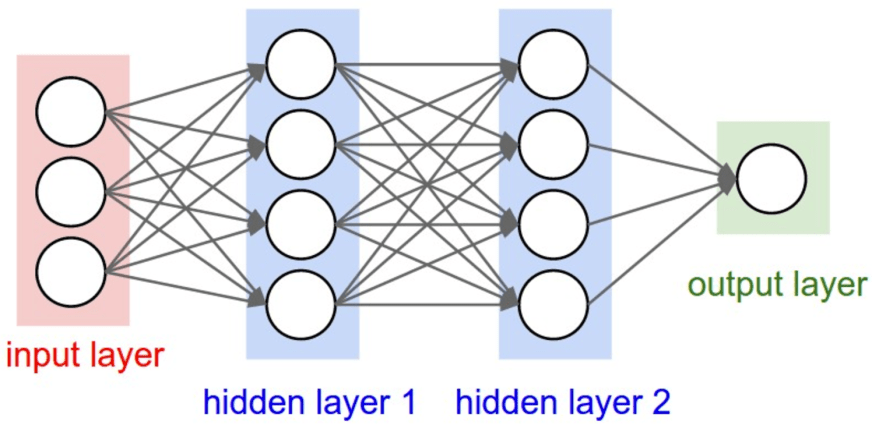
Now you don’t have to know anything about the math, or coding to comprehend this. This isn’t a tough concept to get your head around. If someone doesn’t know this they don’t have enough interest to Google the basics of machine learning. However, I’ve spoken to clinicians who said that machine learning will never play a role in image diagnosis because the algorithm cannot take into account parameters like obs, past med history, and presenting complaint. What they really should have said is, “I don’t know anything about machine learning, not even the pop science basics. I have not spent more than 10 minutes reading about the basic general concepts that would come up in a Google search.”. This doesn’t just inhibit innovation, it also wastes talent. I know of a junior doctor who can code in python and did neuroscience modeling with the algorithms he coded. This is his story:
“my clinical supervisor meeting for my last placement I said that I wanted to get involved in their data and could code in Python. My supervisor got me clicking through the telemetry to find AF for a week”
We all agree that developers should have someone on the team who understands how a hospital works. However, we also have to admit that if a clinician is having a say about tech innovation, they should understand the basics of computer systems. If you’re a clinician who is not interested in tech, that’s fine, just be honest. What’s not forgivable is a clinician who holds back innovation and wastes resources because they want to protect their ego or image. I’m an advocate for a basic qualification in computer system understanding. If a nurse wants to become a research nurse, they have to sit through an online course on data governance and trial protocol and take a test afterward. A lightweight online course with a test on what a server is, basic computer hardware, what is a high-level language, different types of databases and their advantages and disadvantages, and basic networking questions would separate the posers from the people who are actually interested. It would also prevent wasted resources and inhibition of innovation.
